
SUSPENSION TRAUMA: A LETHAL CASCADE OF EVENTS
DR. NORMAN WOOD June 11, 2012
Updated August 2020

DREW VIGNEULLE
The Vigneulle family has authorized the following of their son in the hope of no other family having to endure such grief.
Drew Vigneulle was a great 25 year old young man. He volunteered to teach kids at camp. Drew was very strong and healthy at 5 feet 4 inches tall and weighed 179 pounds. Drew was an avid rock climber with exceptional upper body strength who traveled the world climbing the most dangerous cliffs. He was an expert in the use of climbing safety harnesses and was very aware of Suspension Trauma.

Drew rocking climbing in Costa Rica.
A few years ago, Drew Vigneulle was deer hunting from his treestand insight of his Alabama home. Drew had his cellphone with him and had been texting his father in the house and had even sent him a video he had taken of himself and the view from his deer stand. When Drew did not arrive back at the house at dark, his father drove out through the field to the treestand. His father found Drew unresponsive, suspended by his harness after he had fallen out of his treestand. Drew had dropped his cellphone.
Drew was found in a seated position with his hands between his legs. Drew’s father called EMS and once they arrived it took them several minutes to get Drew’s body down to the ground. EMS performed CPR and hooked a heart monitor to Drew. But Drew had already passed away. Drew died of positional asphyxia, a form of Suspension Trauma while suspended in his harness.
A few years ago, Drew Vigneulle was deer hunting from his treestand insight of his Alabama home. Drew had his cellphone with him and had been texting his father in the house and had even sent him a video he had taken of himself and the view from his deer stand. When Drew did not arrive back at the house at dark, his father drove out through the field to the treestand. His father found Drew unresponsive, suspended by his harness after he had fallen out of his treestand. Drew had dropped his cellphone.
Drew was found in a seated position with his hands between his legs. Drew’s father called EMS and once they arrived it took them several minutes to get Drew’s body down to the ground. EMS performed CPR and hooked a heart monitor to Drew. But Drew had already passed away. Drew died of positional asphyxia, a form of Suspension Trauma while suspended in his harness.

Drew Vigneulle deceased
When Drew fell, he ended up with most of his body below the level of the treestand platform and Drew with all his strength could not get back up on it. The tree steps were on the other side of the large tree and Drew was not able to reach them.
Drew tried to make his harness into a sit harness like his climbing harness. He moved his leg straps out of his groin to his mid-thighs. Probably to make himself more comfortable and possibly to avoid blood pooling in his legs which can lead to unconsciousness and death. As stated by his father, Drew knew about Suspension Trauma.
When Drew moved his leg straps out of his groin to mid-thigh, his body slid down into the harness into a seated position. This did get the pressure out of his groin, but it increased the pressure around his chest, making it more difficult to breathe. Drew died insight of his home.
The Vigneulle family has graciously given me permission to use Drew’s pictures, and I have named my butt seat strap, the Vigneulle Seat in honor of Drew and what he was trying to do to save his life.
If Drew Vigneulle could not get out of that safety harness, none of us could have. Drew’s harness was not defective, it performed exactly as designed, it stopped his fall. But then what?
Most treestand injuries and deaths occur during the afternoon hunt climbing into or out of the treestand. If you fall in the afternoon or evening, someone may be looking for you after dark. It is extremely hard to find an injured person in the woods after dark. Sometimes, the injured person may not be able to speak.
Make sure you tell someone exactly where you will be hunting. Use a map in your home with pins to pinpoint the exact location of your treestand in case someone needs to come and find you.
It is highly recommended to use a Vertical Safety Line with Prusik Knot (not included) anytime you are climbing into or leaving the treestand. You should have your harness tether connected to a Prusik Knot on the Vertical Safety Line from the time you leave the ground until you get back to the ground.
A Prusik Knot will allow you to be connected to the Vertical Safety Line and slide the Prusik Knot up or down the Vertical Safety Line as you climb up the tree or back down. If you fall while climbing, the Prusik Knot will tighten on the line and prevent you from falling further.
While climbing always have 3 points of contact with your steps or ladder. Either two hands and one foot or two feet and one hand. This will help ensure your safety while climbing.
SUSPENSION TRAUMA
In 2009, the Bureau of Labor Statistics estimated that there were over 212,000 industrial related falls that resulted in serious injury, 605 fatalities. Over the years, these numbers have stayed very consistent. That averages 48 falls per hour if considering a 12-hour work day and a work year of 365 days. Occupational Safety and Health Administration (OSHA) has stated that falls are the leading cause of construction death and the second leading cause of workplace injuries. The Consumer Product Safety Commission, CPSC, estimates that there are approximately 6000 treestand related injuries each year to hunters.
After a successful fall stop with a full body harness, a person will feel the obvious elation of still being alive. But if immediate recovery back to a standing position is not possible, another less known lethal danger must be responded to very quickly; and it is called Suspension Trauma
When Drew fell, he ended up with most of his body below the level of the treestand platform and Drew with all his strength could not get back up on it. The tree steps were on the other side of the large tree and Drew was not able to reach them.
Drew tried to make his harness into a sit harness like his climbing harness. He moved his leg straps out of his groin to his mid-thighs. Probably to make himself more comfortable and possibly to avoid blood pooling in his legs which can lead to unconsciousness and death. As stated by his father, Drew knew about Suspension Trauma.
When Drew moved his leg straps out of his groin to mid-thigh, his body slid down into the harness into a seated position. This did get the pressure out of his groin, but it increased the pressure around his chest, making it more difficult to breathe. Drew died insight of his home.
The Vigneulle family has graciously given me permission to use Drew’s pictures, and I have named my butt seat strap, the Vigneulle Seat in honor of Drew and what he was trying to do to save his life.
If Drew Vigneulle could not get out of that safety harness, none of us could have. Drew’s harness was not defective, it performed exactly as designed, it stopped his fall. But then what?
Most treestand injuries and deaths occur during the afternoon hunt climbing into or out of the treestand. If you fall in the afternoon or evening, someone may be looking for you after dark. It is extremely hard to find an injured person in the woods after dark. Sometimes, the injured person may not be able to speak.
Make sure you tell someone exactly where you will be hunting. Use a map in your home with pins to pinpoint the exact location of your treestand in case someone needs to come and find you.
It is highly recommended to use a Vertical Safety Line with Prusik Knot (not included) anytime you are climbing into or leaving the treestand. You should have your harness tether connected to a Prusik Knot on the Vertical Safety Line from the time you leave the ground until you get back to the ground.
A Prusik Knot will allow you to be connected to the Vertical Safety Line and slide the Prusik Knot up or down the Vertical Safety Line as you climb up the tree or back down. If you fall while climbing, the Prusik Knot will tighten on the line and prevent you from falling further.
While climbing always have 3 points of contact with your steps or ladder. Either two hands and one foot or two feet and one hand. This will help ensure your safety while climbing.
SUSPENSION TRAUMA
In 2009, the Bureau of Labor Statistics estimated that there were over 212,000 industrial related falls that resulted in serious injury, 605 fatalities. Over the years, these numbers have stayed very consistent. That averages 48 falls per hour if considering a 12-hour work day and a work year of 365 days. Occupational Safety and Health Administration (OSHA) has stated that falls are the leading cause of construction death and the second leading cause of workplace injuries. The Consumer Product Safety Commission, CPSC, estimates that there are approximately 6000 treestand related injuries each year to hunters.
After a successful fall stop with a full body harness, a person will feel the obvious elation of still being alive. But if immediate recovery back to a standing position is not possible, another less known lethal danger must be responded to very quickly; and it is called Suspension Trauma

OSHA requires that a suspended worker be rescued “As quickly as possible”, presumably within 10 minutes. They further state, “Suspension in a fall arrest system can result in unconsciousness, followed by death, in less than 30 minutes”. ANSI Z359.2 states that contact with a suspended worker must be within 6 minutes.
In 2009, the Consumer Product Safety Commission (CPSC) stated in a letter to the Treestand Manufactures Association (TMA) that the use of a Suspension Relief Strap is not self-rescue. These decisions and rulings are not haphazardly determined; they are based on 40 years of research and studies conducted on harness safety and Suspension Trauma.
In 1972, during the Second International Conference of Mountain Rescue Doctors, an Austrian report was discussed in which 10 climbers had become suspended and had to be rescued. Some were using foot loops for suspension relief straps.
The Rescues took anywhere from 30 minutes to 8 hours. Two climbers died before help arrived, three died shortly after being rescued and the other five died over the next 11 days. None had any external signs of significant injury. They all died from Suspension Trauma but from different mechanisms of pathophysiology, which will be explained shortly.
The Innsbruck Mountain Rescue Service in Austria decided to do additional circulatory and renal testing after a review of the Austrian Report. They took 10 experienced rescue personnel and suspended all of them in their Sit harnesses and foot slings (suspension relief straps). They were instructed not to move.
The test was to proceed for a minimum of 30 minutes. Three test subjects passed out before reaching 30 minutes and had to be revived. The test was stopped shortly after 30 minutes for the other seven test subjects. All these test subjects survived without long term injury.
In concluding remarks on the papers of the Second International Conference of Mountain Rescue Doctors it was stated by the authors; “Orthostatic shock and typical respiratory obstruction may lead to death when hanging on a rope; the probability of survival after hanging two hours is small; death may occur during or after detachment from the rope when rescued.”
In 1987, at the request of OSHA, the United State Air Force conducted extensive harness suspension testing at the Wright Patterson Air Force Base, Ohio. Thirteen test subjects were given a comprehensive medical evaluation and screening before entry into the test group. Final test results showed that an immobile person suspended in a full body harness has an average physical tolerance limit of 14.5 minutes before exhibiting presyncopal or near fainting symptoms at which time the test was terminated.
Presyncopal symptoms included nausea, light headedness, peripheral vision loss, flushing and paresthesia of the extremities. The range of tolerance limits from 5 to 30 minutes were observed before testing was terminated. It was also noted that a person suspended in a vertical position is in danger of brain damage and eventual death within 4 to 6 minutes of fainting.
In 1997, NASA conducted a study on orthostatic intolerance in astronauts. During the study, one test subject became unconscious in 3 minutes. This study was the foundation for the article “Will Your Safety Harness Kill You?” by Dr. Bill Weems and Dr. Phil Bishop, OHS, March 2003.
For over 2000 years’ man has known that being suspended in a vertical position with the legs immobile can cause death. In the Bible, references to the death of Jesus Christ indicate that he died between three and six hours. Crucifixion victims ultimately died of Suspension Trauma induced pathology, the customary breaking of the legs, only hastened the outcome.
In 2009, the Consumer Product Safety Commission (CPSC) stated in a letter to the Treestand Manufactures Association (TMA) that the use of a Suspension Relief Strap is not self-rescue. These decisions and rulings are not haphazardly determined; they are based on 40 years of research and studies conducted on harness safety and Suspension Trauma.
In 1972, during the Second International Conference of Mountain Rescue Doctors, an Austrian report was discussed in which 10 climbers had become suspended and had to be rescued. Some were using foot loops for suspension relief straps.
The Rescues took anywhere from 30 minutes to 8 hours. Two climbers died before help arrived, three died shortly after being rescued and the other five died over the next 11 days. None had any external signs of significant injury. They all died from Suspension Trauma but from different mechanisms of pathophysiology, which will be explained shortly.
The Innsbruck Mountain Rescue Service in Austria decided to do additional circulatory and renal testing after a review of the Austrian Report. They took 10 experienced rescue personnel and suspended all of them in their Sit harnesses and foot slings (suspension relief straps). They were instructed not to move.
The test was to proceed for a minimum of 30 minutes. Three test subjects passed out before reaching 30 minutes and had to be revived. The test was stopped shortly after 30 minutes for the other seven test subjects. All these test subjects survived without long term injury.
In concluding remarks on the papers of the Second International Conference of Mountain Rescue Doctors it was stated by the authors; “Orthostatic shock and typical respiratory obstruction may lead to death when hanging on a rope; the probability of survival after hanging two hours is small; death may occur during or after detachment from the rope when rescued.”
In 1987, at the request of OSHA, the United State Air Force conducted extensive harness suspension testing at the Wright Patterson Air Force Base, Ohio. Thirteen test subjects were given a comprehensive medical evaluation and screening before entry into the test group. Final test results showed that an immobile person suspended in a full body harness has an average physical tolerance limit of 14.5 minutes before exhibiting presyncopal or near fainting symptoms at which time the test was terminated.
Presyncopal symptoms included nausea, light headedness, peripheral vision loss, flushing and paresthesia of the extremities. The range of tolerance limits from 5 to 30 minutes were observed before testing was terminated. It was also noted that a person suspended in a vertical position is in danger of brain damage and eventual death within 4 to 6 minutes of fainting.
In 1997, NASA conducted a study on orthostatic intolerance in astronauts. During the study, one test subject became unconscious in 3 minutes. This study was the foundation for the article “Will Your Safety Harness Kill You?” by Dr. Bill Weems and Dr. Phil Bishop, OHS, March 2003.
For over 2000 years’ man has known that being suspended in a vertical position with the legs immobile can cause death. In the Bible, references to the death of Jesus Christ indicate that he died between three and six hours. Crucifixion victims ultimately died of Suspension Trauma induced pathology, the customary breaking of the legs, only hastened the outcome.

Tilt table testing has confirmed that even in the absence of being suspended in a harness, hypotension, bradycardia and presyncopal symptoms can occur in 80% of healthy adults in less than one hour. These same symptoms have been recorded in EMS training exercises where a healthy subject was immobilized on a backboard and carried feet first down flights of stairs. It is very common for military personnel to pass out while standing at attention. Gravity and immobility is all that is required for a syncopal event to occur in a vertically positioned person; being suspended in a harness makes unconsciousness occur quicker and it can be lethal.

Tilt Table Testing
|

Gravity and Immobility is all that is required for Blood Pooling to occur
|
It is very evident that body posture, health of the individual, immobility, gravity, body weight, vasovagal responses to pain, emotional stress, hypovolemia, hypotension, bradycardia, cerebral hypoxia, dehydration, exhaustion, confusion, panic, hypoglycemia, restrictive respiration, and obstruction to blood circulation all play important roles in the Suspension Trauma Cascade of injury and death.
Over the past 40 years, study after study has confirmed that being suspended in certain types of harnesses accelerate the onset of syncopal events and Suspension Trauma. A full body harness can allow for a life-saving experience, but immediately upon suspension, time can quickly run out in a matter of minutes due to the rapid activation of the Suspension Trauma Cascade of events. If this cascade is allowed to progress, a suspended person will experience each and every one of these events, including death.
In an overall view of Suspension Trauma, one must mention the liability aspects of training, equipment and the personal safety of employees and consumers. “Failure To Warn” litigation has been a very costly endeavor for companies in the past. Failure To Warn has been ruled negligence by the courts and multi-million dollar settlements have been common.
“During your official capacity and in the course of instructing or advocating the use of any product, you MUST provide complete information and inform of ANY potential dangers in using that product if there is ANY possibility of it causing injuries”. This description of Failure To Warn, lays out the heart of the matter; there are moral, ethical and legal responsibilities that must be adhered to for personal safety, and if not stringently followed, the cost of litigation will only be outweighed by the cost in human life.
HARNESS TYPE AND SUSPENSION TRAUMA FACTORS
A distinction needs to be made between a front-attached work harness similar to an Alpine, Climbing or an Arborist Sit harness, and a rear-attached safety harness that is used in construction and hunting from treestands.
A front-attached Alpine, Climbing or Sit work harness is designed for the user to be suspended in them while they work; the very design of these harnesses cause very little pressure against the femoral veins in the legs which are located in the anterior groin. These are the main vessels that return blood from the legs. Also, while suspended in this type of harness, the upper sections of both legs are in more of a horizontal position helping to negate the gravitational pull on the blood.
Over the past 40 years, study after study has confirmed that being suspended in certain types of harnesses accelerate the onset of syncopal events and Suspension Trauma. A full body harness can allow for a life-saving experience, but immediately upon suspension, time can quickly run out in a matter of minutes due to the rapid activation of the Suspension Trauma Cascade of events. If this cascade is allowed to progress, a suspended person will experience each and every one of these events, including death.
In an overall view of Suspension Trauma, one must mention the liability aspects of training, equipment and the personal safety of employees and consumers. “Failure To Warn” litigation has been a very costly endeavor for companies in the past. Failure To Warn has been ruled negligence by the courts and multi-million dollar settlements have been common.
“During your official capacity and in the course of instructing or advocating the use of any product, you MUST provide complete information and inform of ANY potential dangers in using that product if there is ANY possibility of it causing injuries”. This description of Failure To Warn, lays out the heart of the matter; there are moral, ethical and legal responsibilities that must be adhered to for personal safety, and if not stringently followed, the cost of litigation will only be outweighed by the cost in human life.
HARNESS TYPE AND SUSPENSION TRAUMA FACTORS
A distinction needs to be made between a front-attached work harness similar to an Alpine, Climbing or an Arborist Sit harness, and a rear-attached safety harness that is used in construction and hunting from treestands.
A front-attached Alpine, Climbing or Sit work harness is designed for the user to be suspended in them while they work; the very design of these harnesses cause very little pressure against the femoral veins in the legs which are located in the anterior groin. These are the main vessels that return blood from the legs. Also, while suspended in this type of harness, the upper sections of both legs are in more of a horizontal position helping to negate the gravitational pull on the blood.

|

|
Front-Attached Sit Safety Harness Minimal pressure on the Femoral Veins
located in the groin area.
Front-Attached Sit Harness Design Ensures Very Little Pressure Placed On The Femoral Veins
located in the groin area.
Front-Attached Sit Harness Design Ensures Very Little Pressure Placed On The Femoral Veins

Both of these qualities in conjunction with active movement of the legs and body allow for a comfortable suspension with less incidence of blood pooling and Suspension Trauma injury or death. Even though blood pooling can occur, the length of time that one can be safely suspended without injury is greatly increased as long as there is active movement. The Hybrid Sit Harness while using the sternal-attachment does not provide the same level of safety as the waist-attachment location. A sternal-attachment is not intended for prolonged suspension and presents similar hazards to a rear-attached harness.
A rear-attached safety harness commonly used in construction and by treestand hunters is not intended to provide long term suspension. Its sole purpose is to provide a fall stop and then one must remove themselves from the harness as soon as possible. When suspended in a rear-attached harness, the Suspension Trauma Cascade begins immediately. With this type of harness, there is direct pressure placed on the femoral vein and nerve from the leg straps, and the legs are hanging in a vertical position allowing for an increased effect of the gravitational pull on the blood.
A rear-attached safety harness commonly used in construction and by treestand hunters is not intended to provide long term suspension. Its sole purpose is to provide a fall stop and then one must remove themselves from the harness as soon as possible. When suspended in a rear-attached harness, the Suspension Trauma Cascade begins immediately. With this type of harness, there is direct pressure placed on the femoral vein and nerve from the leg straps, and the legs are hanging in a vertical position allowing for an increased effect of the gravitational pull on the blood.

|
|
Rear-Attached Safety Harness Leg Straps Exert Direct Compression On The Femoral Vein
While suspended, a restrictive force is also placed against the abdominal and thoracic areas increasing the difficulty in breathing and discomfort. A rear-attached harness is very difficult to move in and will drain all your energy to exhaustion very quickly. In personal testing and harness development over the past 15 years involving thousands of suspensions, my personal exhaustion limit in trying to recover to a standing position is reached in less than 5 minutes. The presyncopal or Suspension Trauma symptoms of tachycardia, nausea, shortness of breath and a feeling of increasing anxiety are felt in less than 12 minutes. I do not believe that I could remain conscious for more than 15 minutes while suspended in a rear-attached harness.
All of these factors result in immediate pooling of blood in the legs, a very rapid deterioration of overall blood circulation, decrease oxygenation of visceral organs, heart and brain, and an increasing level of physical discomfort and emotional stress. These immediately combined factors support the progression of the Suspension Trauma Cascade which is responsible for a suspended victim becoming symptomatic very quickly and losing consciousness.
SUSPENSION TRAUMA CASCADE
While suspended in a safety harness, the leg straps cause a tourniquet effect on the femoral vein and pressure on the femoral nerve, causing blood to pool in the lower extremities, and considerable discomfort and pain. The venous return from the legs has very little pressure behind it, approximately 1/5 of the arterial pressure going into the legs. During ambulation, the normal venous pressure in the feet of 25 mm Hg can be increased to 90 mm Hg in just a few minutes due to gravitational pull on the blood and immobility.
To assist the body in movement of blood against gravity, the venous return from the legs has one-way valves to help the transfer of blood back to the heart. To provide the pressure needed to overcome the gravitational pull on the blood, active leg muscle contractions must be used. As the leg muscles contract, pressure is exerted on the veins in the legs forcing the blood through the one-way valves and back to the heart.
Unfortunately, while suspended in a harness, the “muscle pumps” of the legs may be inadequate to overcome the compressive forces placed on the femoral veins by the leg straps and blood pooling occurs. Even with active leg movements, which can prolong the onset of presyncopal symptoms, they ultimately may be ineffective against the rapidly progressing chain of events that cause increasing immobility and unconsciousness.
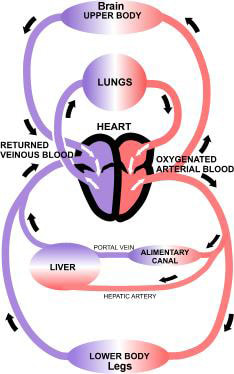
Normal Circulation
|
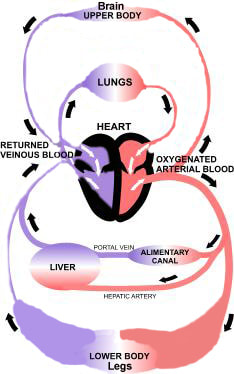
Blood Pooling
|
There are many reasons why a suspended person would become immobile; a lack of understanding of Suspension Trauma, injury, confusion, physical and emotional exhaustion, pain, hypoglycemia, muscle failure due to hypoxia and aesthesia of the legs, or the Suspension Trauma Cascade has progressed to the point of unconsciousness. The longer the suspension, the less mobile a person will become and the Suspension Trauma Cascade of events will begin to proceed at an ever-progressive rate.
The average human body contains 10 pints of blood with two pints normally in the legs at any one time. As soon as a person is suspended in a rear-attached harness, those two pints of blood are trapped in the legs and the body has a decrease of 20% of its total circulating blood volume and Class II Hypovolemic Shock is present. The heart is powerful enough to push the blood past the leg straps via the arteries and as long as the heart continues to beat, more blood will be pushed into the legs where it will be trapped.
The lower extremities can hold 60% (6 pints) of a body’s total blood volume. As soon as the heart has pumped over 40% (4 pints) of blood into the legs, the victim is now in Class IV Hypovolemic Shock, the most severe level of Hypovolemic Shock with impending death if no immediate medical care is rendered. There is no Class V.
This is the same as cutting both wrists and bleeding out half of the body’s blood. Blood pressure and oxygen levels drop to a critical point where it causes unconsciousness and then death. If the body is placed in a horizontal position, survival is possible; however, being suspended by a harness in a vertical position, there is little chance of survival without immediate suspension relief.
A Vasovagal syncopal event, fainting, while suspended in a vertical posture can end in the same catastrophic result. The Autonomic Nervous System, ANS, controls our “Fight or Flight” responses as well as our “Normal Relaxation State”. In an emergency, similar to having a harness fall stop, the sympathetic or “Fight or Flight” component of the ANS quickly prepares us to physically respond by increasing the heart rate, breathing and blood pressure through catecholamine release and blood vessel constriction.
This sympathetic control will remain dominate in an emergency unless reduced by an increasing parasympathetic tone. The parasympathetic or “Normal Relaxation State” component of the ANS creates the opposite effect on the body by decreasing the heart rate and blood pressure. The 10th Cranial Nerve, the Vagus Nerve is part of the parasympathetic ANS.
The Vagus Nerve can be stimulated by pain, emotional stress and hypovolemia. While suspended in a harness the body can be experiencing all three stimulants and the longer the suspension, the more intense the vagal tone will become. Contributing to this vasovagal event is the Bezold-Jarisch Reflex which is initiated when ischemic hypoperfusion or hypovolemia is sensed by chemoreceptors and mechanoreceptors in the left ventricle of the heart. This reflex causes a marked increase in vagal tone causing immediate bradycardia and dilatation of blood vessels by decreasing the sympathetic input.
When the vagal tone becomes significant enough, a vasovagal syncopal event will occur due to the rapidly decreasing heart rate, blood pressure, and cerebral perfusion. This can take a minute or two where the victim feels the symptoms of presyncope, or it can be instantaneous as in a person fainting over the sight of blood or being stuck by a needle. A victim will never know how soon this event will occur, but it will be very rapid.

Vasovagal Event (Fainting)
Elements of the Suspension Trauma Cascade can present so suddenly that the suspended victim may have little opportunity to respond in an effective manner. One of the earliest symptoms of Suspension Trauma is cognitive impairment or confusion which makes the suspended victim much less likely to be able to assist in their own self rescue.
As soon as the Suspension Trauma Cascade progresses to the victim’s limits of physical or emotional tolerance, unconsciousness will occur by hypovolemic shock, vasovagal event, or both. During unconsciousness, the respiratory rate will slow, oxygenation of the brain and heart will diminish, thus causing a greater drop in respiration and blood pressure which causes a further drop in oxygenation and the cascade spirals downward. There will be permanent brain damage in a few minutes. The heart will stop shortly after that when it sustains a global myocardial infarction, a “massive heart attack” from the lack of oxygen and death occurs. All of this can happen in “less than 30 minutes”.
HOW THE 10 VICTIMS FROM THE AUSTRIAN REPORT POSSIBLY DIED
Recall that these victims had prolonged suspensions anywhere from 30 minutes to 8 hours before being rescued, some of whom had Suspension Relief Straps. All of them were in front-attached harnesses or rope slings.
The two that died before being rescued may have succumbed to the classic cascade of events associated with Suspension Trauma. Either hypovolemic shock, when excessive blood pooled in the legs, or a vasovagal syncopal event occurred. With either, blood pressure and brain oxygenation will drop to a critical level where the victim becomes unconscious and death quickly follows.
The three victims that died shortly after being rescued may have died of sudden cardiac arrest or pulmonary emboli. This can be caused by hypoxic injury to the myocardium while suspended and by the blood which was once pooled in the legs becoming a toxic sludge which consist of low oxygen levels, blood clots and high potassium (hyperkalemia). The third and final injection during a Lethal Injection Execution is potassium, it stops the heart.
While suspended in a harness, the extent of stasis that the blood is exposed to will determine the degree of pathological changes that occur to that collection of blood. If the venous return is only slowed as in a sit harness with increasing immobility, the pathological changes in the pooled blood of the legs will take longer to occur, perhaps hours. If the venous return is stopped or near so as in a rear-attached safety harness, the pathological changes will begin to occur immediately.
As blood pooling continues in the legs, increasing hypoxia within the stasis blood triggers anaerobic metabolism in the muscle cells. Lactic acid, a byproduct of anaerobic glycolysis, causes the pooled blood to become increasingly acidotic. During an acidotic state, an ionic shift will occur between the hydrogen ions in the blood and potassium ions in the muscle cells causing the pooled blood to become hyperkalemic. Damaged Red Blood Cells will also release their own potassium.
As the pooled blood becomes more hypoxic and stagnant, micro blood clot formation will begin very quickly which can lead to Deep Vein Thrombosis, DVTs. When the movement of blood, circulation, is stopped this imitates death to that section of the body. Anyone that has harvested a game or farm animal and then immediately cleaned that animal has observed the clot formation that has already accumulated. This same process of pathological change occurs in the stasis blood of the legs while suspended. Clot formation is easily observed in this instance, what cannot be visually observed is the pathological changes of the chemical composition of the blood to an acidotic state with high potassium and low oxygen content.

Blood Clot Formation Beginning in Pooled Blood after 10 minutes

Well Formed Blood Clot in Pooled Blood after 20 minutes

Blood Clot completely formed in Pooled Blood after 30 minutes
At 10 minutes, the pooled stasis blood is already starting to form clots. The scattered dark spots are the micro clot formation and the thickened area is more advanced clot formation. Although troublesome, a person would have a good chance of survival if this blood was allowed to circulate back to the heart and lungs. At 20 and 30 minutes, these clots are well formed and are potential killers and if allowed to circulate back to the heart and lungs, death can occur in less than one minute.
The pathological chemical changes occur at the same time and for the same reasons that clot formation begins and depending on the type of harness suspended in and the length of time of suspension, over half of a person’s total blood volume may become incompatible with life. Once the tourniquet effect of the leg straps is removed, this blood can rapidly return to the heart, causing it to go into a fatal arrhythmia and/or clots can be shed to the lungs, either of which can kill a victim very quickly.
The victims that died shortly after being rescued may have been laid down in a supine position, which is considered the standard of care for trauma victims; however, this can be detrimental if the conscious and alert victim has been suspended for a prolonged period of time. It must be remembered that a suspended person is not a typical trauma victim. They have not fallen to the ground, they have been suspended, a very unique circumstance. On site EMS care must be adjusted and is discussed later.
The final five may have died over the next few days of hypoxic damage sustained by the heart, pulmonary emboli or acute kidney failure. The kidneys cannot tolerate low blood flow and low oxygen levels caused by blood pooling while hanging suspended in a harness. Renal tubular necrosis is the kidney “rotting from the inside out” and is caused by hypoperfusion while suspended.
The kidneys can also be damaged by myoglobin, a large muscle protein released in the blood when muscle cells begin to break down in a low oxygenated state and from leg strap compression injury, a condition called Rhabdomyolysis. These bulky proteins obstruct the fine membranes of the filtration system of the kidneys causing acute kidney failure.
It can take a day or two before acute kidney failure becomes significant enough to make the victim ill. A short period of no symptoms may precede the acute onset of kidney failure which can quickly lead to death. 50% of all acute kidney failure victims die.
CONSIDERATIONS
It is very clear from all available reports and studies conducted on Suspension Trauma and from the medical knowledge of the pathophysiological effects on the body, a person will never know how much time he will have to survive and even if rescued after being suspended for a prolonged period of time, that victim is still in very grave danger of serious injury or death. Suspension Trauma can be quickly lethal and anyone using a rear-attached full body harness must be aware of the dangers and use all precautions.
That being said, if you do not wear a full body harness and fall, your odds of survival may be zero. Even if you survive, you may still sustain catastrophic injuries where any further employment is impossible for the rest of your life. Always wear a full body harness and use all available safety measures.
SUSPENSION RELIEF
There have been documented accounts where workers have fallen and been suspended in their harnesses for over an hour while using a Suspension Relief Strap, SRS, with no long term affects.

Suspension Relief Strap takes pressure off of the Femoral Vein
The Suspension Relief Strap should be PERMANENTLY attached to your harness. It is useless if it is not with you at all times. A non-attached SRS can be left at home or in your vehicle. Not having it permanently attached to you harness can cost you your life. Also, a non-permanently attached SRS can be dropped while trying to use it in a panicked emergency situation with shaking hands, an injured victim, or in low light conditions. If you drop it, that can cost you your life.
If you do find yourself suspended, deploy the SRS immediately, if recovery back to a standing position is not possible. Do Not Wait! If you have not recovered to a standing position in 30 seconds, you probably will not be able too, that is the time to use the Suspension Relief Strap.
A Suspension Relief Strap that allows you to place BOTH of your feet in it for support is much more effective than a single foot design. As we have mentioned, you must have muscle contractions to assist the blood from your legs and back to your heart by the one-way valves in the leg veins. With a two-foot design, you can maximize the blood flow return by rhythmically placing your bodies weight on one foot and then the other as if you are walking. These muscle contractions put pressure on the leg veins and forces the blood back to the heart because of the one-way valves, the blood can only go in one direction and that is up. This allows for increased blood to return from the legs to the heart, and will allow you more time to hopefully survive until rescued. This will not be comfortable, but it will maximize your chances of survival.
A single-footed Suspension Relief Strap is not effective because of the following reasons; When you stand in a single-footed SRS, you must contract your leg musculature in that one supporting leg to stand. You must also continue to contract the musculature in that one leg to continue standing. To pump blood out of your leg, you must be able to relax the muscles to allow for more blood to enter the veins as the blood tries to seep upward. While you are standing on that one foot, contracting the muscle of that one leg, you have given yourself ONLY ONE MUSCLE PUMP. You must have the ability to relax the muscle of the supporting leg to allow for more blood to enter into the venus system and then contract the muscle again to force the blood back to the heart via the one-way valves. As long as you stand on that one leg, you will continue to have ONLY ONE MUSCLE PUMP because you are constricting the vessels while the leg muscles are contracted.
While you are on one foot, the other non-weight bearing leg muscles are NOT contracted, so the non-weight bearing leg is not assisting in the muscle pump at all to help circulate blood back to the heart and lungs. Therefore, a single-foot Suspension Relief Strap is not recommended. If you find yourself in a suspended state and you are unfortunate to only have a single-foot SRS, do not alternate your feet!
By alternating your feet, you make the single-footed SRS even less effective, this is why; When you alternate feet, you are wasting time and muscle pumps. To alternate feet, you must sit back down in the harness, take the single-foot SRS off one foot and place it on the other while you are suspended. It may be dark, or you may have a large abdomen, or you may have work boots on, but it will take considerable time to switch feet. While you are seated in your harness and trying to switch feet, with every beat of your heart, you are sending more blood to your legs where it is trapped by the leg straps and cannot return. With every beat of your heart, you send several ounces of blood to your legs. How many heart beats do you think it will take for you to sit down, take one foot out of the SRS and place it on the other and then stand back up to get ONE MORE MUSCLE PUMP? Several heart beats for sure.
If you have a single-footed SRS, DO NOT CHANGE FEET!!! Stand up, sit back down in the harness, and stand back up on the same foot. As fast as you have read this, you could have had TWO MUSCLE PUMPS from that same leg. While you do this either use Isometric contractions of the muscle of the non-weight-bearing leg, or place the not used foot on top of your slinged foot and press down with each stand. Your heart, lungs and brain do not care what leg the blood comes from, it only cares if it gets blood. So you must maximize the pumping of blood from your legs and changing feet takes too much time.
This is the same reason why military personnel are trained NOT to lock their knees while standing in formation. By locking your knees, you must contract the upper leg muscles and this puts constant pressure on the upper leg veins and it continues to restrict blood from seeping upward. By not locking your knees, you are not giving it muscle pumps, but at least you are not restricting the blood flow unnecessarily. Even when not locking your knees, many personnel still pass out from the blood pooling while not moving their legs. The force of gravity may be stronger than your return seep
STATISTICS
Trauma center statistics on fall victims are well known and they are startling. 80% will require surgery, 60% will have fractures, 30% will have spinal fractures and 10% will have permanent disabilities or paralysis. And a significant number of fall victims will die. The use of a full body harness is mandatory in industry and construction for these very reasons and one should be mandatory while hunting from a treestand as well.
Not to use a full body harness while in an elevated position is a foolhardy decision that may cost you and your family dearly. When you are in an elevated position, your entire family is with you. Whatever happens to you will directly affect all of them. The odds of you falling are significant. Be aware of the dangers of Suspension Trauma, and always use a full body harness and be connected from the time you leave the ground until you get back down. Safety first, everybody needs to go home to their families.
WHAT TO DO IF CAUGHT SUSPENDED IN YOUR HARNESS AND RECOVERY BACK TO A STANDING POSITION IS NOT POSSIBLE
DO’S
1-Make sure you have told someone where you will be at all times.
2-If you are using a descending harness or device, immediately lower yourself to the ground. You need to get to the ground or to a standing position as soon as possible because Suspension Trauma can cause you to lose consciousness in less than 30 minutes and death will shortly follow unconsciousness.
3-If you are wearing a traditional harness, use your Suspension Relief Strap immediately, within 30 seconds. A suspension relief strap can slow the Suspension Trauma cascade if used quickly. A double-footed permanently attached SRS is superior, it will allow you to rhythmically pump both legs to assist in pumping the blood out of your legs and back to your heart. If you have a single-foot SRS, keep it on the same foot and continue to stand repeatedly from a seated position as rapidly as you can. Use Isometric contractions on your non-weight-bearing leg or place that foot on top of your slinged foot and press down with each stand. If you do not have a permanently attached SRS, always keep it on your body in case it is needed!
4-After standing in the Suspension Relief Strap, you may need to loosen the leg straps slightly to help blood circulation. Do not remove them.
5-KEEP YOUR LEGS MOVING, active muscle contractions are the only way to pump the blood from your legs back to your heart through the one-way valves in the leg veins. Move your legs like your life depends on it, because it really does.
6-If you do not have a Suspension Relief Strap, DO NOT LOOSEN YOUR LEG STRAPS OR MOVE THEM OUT OF YOUR GROIN. If you do, your body can side down into the harness, placing more pressure on your abdomen and chest, causing you not to be able to breathe effectively. Although painful, you may be able to survive longer with pressure in your groin area than on your abdomen or chest. Try to place your feet against an object to contract your leg muscles to help pump blood from your legs.
7-Try to eliminate any pressure points that are causing pain. Pain can cause a vasovagal or fainting episode. A vasovagal episode can be created by pain, emotional stress or hypovolemia; all three may be present while suspended in a harness. If you pass out the probability of death greatly increases.
8-Get help as soon as you can, blow a whistle, call on a cell phone or yell.
9-If rescued, conscious and alert, STAY IN A SEATED POSITION FOR AT LEAST 45 MINUTES. Do not lie down; it can cause a fatal arrhythmia. Being seated will allow the slow reintroduction of the pooled blood back into circulation. Move your legs gently to help restore the circulation. Do not walk for 45 minutes.
10-GO TO THE HOSPITAL and tell them you have been suspended and may have heart or kidney damage. You may need dialysis to prevent kidney failure or death.
11-Make sure you have repeat blood work in 2 days. Remember that acute kidney failure may take a day or two to present.
DON’T’S
1-Don’t panic, you must use your head, try to stay calm. Think about how you can safely release yourself from the suspended state.
2-DON’T STOP MOVING YOUR LEGS; doing so may increase the chance of death. Take short breaks but keep moving those legs.
3-Don't allow yourself to become exhausted; pace yourself. You may be suspended for a long time.
4-Don't pass out; your survival depends on it. Fight it!
5-DON'T LAY DOWN IF RESCUED; remain in a seated position for at least 45 minutes. This will allow the pooled blood in the legs to be slowly reintroduced back into circulation.
6-DON’T GO HOME, GO TO THE HOSPITAL!
7-DON’T BE FOOLED; If released from the hospital, have repeat blood work in 2 days to recheck kidney function.
EMS RESCUE PROTOCOL OF A SUSPENDED VICTIM
It is important to remember that a victim of Suspension Trauma is not a typical “trauma” victim. The EMS standard of care of supine positioning for trauma victims may prove fatal if a conscious victim has been suspended for a prolonged period of time. Positioning of the victim is critical to allow for the slow reintroduction of the pooled blood back into the circulation. The longer the suspension the more critical post-suspension positioning becomes.
1-GET THEM DOWN AS SOON AS POSSIBLE! Time is of the essence, the only way to assist a victim is to get them out of the suspended state ASAP!
2-IF CONSCIOUS AND ALERT, place the victim in a seated or Fowler’s position for at least 45 minutes to allow for the slow reintroduction of the pooled blood back into the circulation. A victim should only gently move the legs to help restore circulation. Do not allow them to ambulate.
3-IF SEMI-CONSCIOUS OR UNCONSCIOUS , you MUST place them in a horizontal (supine) position to help restore blood flow to the brain and prevent any further brain damage from hypoxia. If the victim becomes conscious and alert, slowly return them to a seated position as tolerated.
4-Oxygen, remember the ABCs: Airway, Breathing, and Circulation.
5-Monitor Cardiac Rhythm, Vitals and Blood Glucose, BE PREPARED FOR HEART ARRHYTHMIAS. ACLS PROTOCOLS always apply.
6-IV Fluids, Calcium Gluconate 10 ml of 10% solution IV can help stabilize the myocardium and counter the hyperkalemic affect.
7-Insulin R 10U with 50 ml D50W IV and Albuterol, can lower the hyperkalemia and counteract hypoglycemia.
8-Sodium Bicarb, counters acidosis.
9-Aspirin, have victim chew one, can help prevent further clot formation. The benefit outweighs the minimal acidotic affect.
10-Get the victim to a facility that has dialysis capabilities.
REFERENCES
1- Bureau of Labor Statistics, U.S. Dept. of Labor. Workplace Injuries, 2009.
2- Occupational Safety and Health Administration. U.S. Dept. of Labor. Fall Safety Standards, 2004.
3- American Standard, ANSI Z359.2, Minimum Requirements for a Comprehensive Managed Fall Protection Program, 2007.
4- Karen M, Consumer Product Safety Commission. Letter to TMA Self Rescue Subcommittee, 2009
5- Seddon P. Harness Suspension: review and evaluation of existing information. Health and Safety Executive. Research Report 451/2002.
6- Orzech M, Goodwin M, Brinkley J, Salerno M, Seaworth J. Test Program To Evaluate Human Response To Prolonged Motionless Suspension In Three Types Of Fall Protection Harnesses. Harry G. Armstrong Aerospace Medical Research Laboratory. Human Systems Division. Air Force Systems Command. Wright-Patterson Air Force Base, Ohio, 1987.
7- Weems B, Bishop P. Will Your Safety Harness Kill You? Occupational Health & Safety Magazine, Vol. 27, March 2003.
8- Barr Y, Fogarty J. Assessment of Prone Positioning of Restrained Seated Crew Members in a Post-landing Stable 2 Orion Configuration. University of Texas Medical Branch Galveston and Wyle Integrated Science and Engineering Group. NASA Johnson Space Center, Houston, 2010.
9- Amphoux M. Translated text from French. Hanging After A Fall, An Extremely Urgent Rescue. International Fall Protection Symposium, Germany, 1998.
10- Lee C, Porter K. Suspension Trauma Review. Emergency Medicine Journal, Vol. 24, 2007.
11- Hollander-Rodriguez J, Calvert J. Hyperkalemia. Oregon Health & Science University, Portland. American Family Physician, Jan, 2006.
12- Agrawal M, Swartz R. Acute Renal Failure. University of Michigan Medical Center, Ann Arbor. American Family Physician, April, 2000.
13- Liano P. Epidemiology of Acute Renal Failure. Kidney International, 1996.
14- Bosch X, Poch E, Grau JM (2009). “Rhabdomyolysis and acute kidney injury”. New England Journal of Medicine 361 (1):62-72. Doi:10.1056/NEJMra0801327. PMID 19571284
15- Mortimer, Roger B, MD. Risks and Management of Prolonged Suspension in an Alpine Harness. Wilderness & Environmental Medicine, 22, 77-86 (2011).